

















Disruption of blood flow and stagnation of blood in the venous bed leads to pathological changes in the blood vessels - varicose veins. The reasons for the onset of the disease can be different, including genetic predisposition (most common), overweight, hormonal imbalance, pregnancy, arterial hypertension, constipation, lifestyle and professional activity (eg work that requires standing for a long time). ).
In all these cases, the development of the disease follows the same scenario and is associated with two factors: the weakness of the vascular wall and the functional insufficiency of the venous valves.
Vascular valves prevent backflow of blood. If they do not succeed in their task, the blood stagnates and accumulates (precipitates) in the veins. As a result, the vessels not only widen, but also lengthen, become tortuous and intertwine into varicose veins.
Most often, this disease affects the superficial veins (large and small) of the lower extremities. They ensure the outflow of venous blood from the subcutaneous tissue and skin, which together make up no more than 1/10 of the total vascular system. The main work is done by the deep veins, connected to the superficial veins through perforating venous channels.
Treatment of varicose veins always means removal or resorption of the vein, that is, its exclusion from the general venous circulation system. But since such ships play a secondary role in this, their removal has no negative consequences. Their function is easily taken over by the remaining veins.

Symptoms and stages of the disease
Varicose veins are one of the most common vascular diseases. According to statistics, 10-20% of men and 30-40% of women suffer from it.
The first signs of pathology are the appearance of a blue or red vascular pattern on the skin. It can be a capillary network or stars (telangiectasia). They most often appear on the legs and thighs, but they can also be found on the face, lips (in women), feet and hands. Spider veins on the face are called rosacea.
Symptoms of varicose veins depend on the stage of the disease. At first it's just heaviness, increased leg fatigue, moderate swelling in the evening, which disappears after rest and sleep. Nocturnal leg cramps are possible.
A characteristic symptom of the disease is pain. Pain in the legs may occur or intensify when walking, standing for a long time or be constant, accompanied by a feeling of fullness, burning and warmth. Varicose veins become painful when pressed.
In international phlebology, the classification of diseases is from class 0 to class 6.
In the zero stage, there are no obvious symptoms; the only complaint could be the heaviness in the legs.
In stage 1, a vascular pattern appears (telangiectasia) and muscle cramps occur at night.
Class 2 disease is manifested by enlarged, thickened veins that protrude under the skin.
In stage 3, the swelling of the legs (ankles, legs, feet) no longer disappears after a night's sleep, a long rest, and becomes persistent.
In the 4th stage, the skin over the varicose veins becomes red or blue, areas of hyperpigmentation appear, skin itching, dryness, peeling and inflammation appear.
Further, in stages 5 and 6, the development of preulcers and trophic skin ulcers follows.
So, varicose veins, which start as an aesthetic problem, can eventually lead to serious health problems.
Complications
Stagnation of venous blood and its accumulation (deposition) in the vessels of the lower extremities causes a decrease in blood pressure, hypotension and associated dizziness, fainting and headaches.
The skin above the affected vessels becomes thinner, inflamed, peeling, itching, congestive dermatitis and varicose eczema, after which trophic ulcers appear.
Blood clots appear in vessels filled with stagnant venous blood, which can break off at any moment and, traveling through the general circulatory system, block a vital artery and lead to death.
In the later stages of varicose veins, complications such as phlebitis and thrombophlebitis develop.
The later the treatment of the disease is started, the greater the risk of its complications, and more radical methods will have to be used to prevent them. Therefore, when the symptoms of varicose veins appear, you should not rely on self-medication, they can be good for prevention. But only a doctor can provide real help.

Diagnosis and treatment
As usual, a visit to the doctor begins with a review of complaints, collection of anamnesis and an external examination. The main method for diagnosing varicose veins is Doppler ultrasound, duplex or triplex ultrasound scanning of blood vessels.
As a rule, this method provides a comprehensive picture of the disease in order to determine the most appropriate treatment tactics.
If additional information is needed to clarify the diagnosis, the doctor may prescribe an X-ray with contrast (radiocontrast venography), MRI of blood vessels (magnetic resonance venography) or multispiral computerized angiography.
Before performing surgical interventions, both minimally invasive and extensive, a standard set of examinations is prescribed - general urine test, general clinical and biochemical blood tests, coagulability test (coagulogram), tests for HIV, syphilis, viral hepatitis, fluorography, EKG.
In most cases, the treatment of varicose veins in a modern clinic is carried out on an outpatient basis or in a day hospital. It does not require a break from everyday life and after only 1-2 hours you can return to your normal activities. Minimally invasive procedures are performed under local anesthesia or without any anesthesia.
And only radical surgical intervention (phlebectomy) may require short-term hospitalization in the inpatient unit of the clinic.
Drug treatment
In the early stages of disease development or for its prevention, the doctor can prescribe drug therapy, including antibiotics and antiseptics (in case of inflammation), phleboprotectors, anticoagulants (to prevent thrombosis), phleboprotectors, heparin ointment and other heparin-containing drugs.
Hirudotherapy can be used as an alternative method of treatment.
Conservative therapy includes wearing compression stockings (socks, ankles) and elastic bandages. It has a limited range.
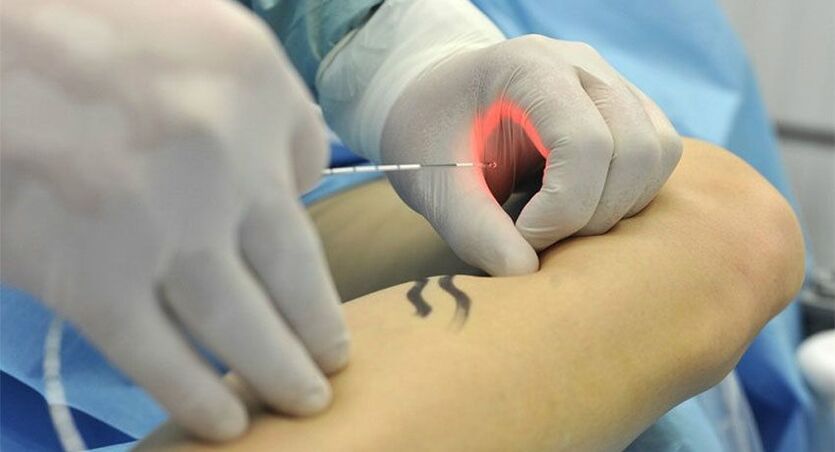
Endovasal laser vascular coagulation (EVLC)
This method refers to minimally invasive methods of treating varicose veins. The procedure is performed on an outpatient basis under local anesthesia. Under ultrasound guidance, a flexible optical fiber connected to an emitting device is inserted into the vascular bed.
Laser light of a certain wavelength is absorbed by blood cells and vein walls and converted into heat.
As a result, the vessel is sealed and turns into a thin bundle of connective tissue that dissolves on its own.
Laser coagulation is commonly used to treat small and medium-sized varicose veins, especially on the face. But with its help you can also eliminate large varicose veins, including small and large leg veins.
Radiofrequency ablation
This method, like EVLC, is based on thermal coagulation, and only radiofrequency radiation, not a laser, is used to close the vessel. Otherwise, the procedure is similar. Under local anesthesia, a radio wave emitter is introduced into the venous bed, which is absorbed by the blood and vascular walls, turns into heat and produces a coagulation effect. The procedure is performed under the supervision of ultrasound.
Like laser coagulation, radiofrequency ablation can be used as the main, only and sufficient method or as part of complex treatment as an additional method. For example, after surgical removal of the main trunk to eliminate minor vascular tributaries.
Sclerotherapy
In this case, the varicose vein is sclerosed - glued from the inside with the help of a sclerosant. This medicine is given into a vein by injection. It can be liquid or foamy.
The procedure is completely painless, and slight stinging and burning may occur during it. To eliminate these sensations, as well as to additionally compress the vessel, a flow of cold air can be used. This is called cryosclerotherapy.
The use of foam sclerosants has a number of advantages. They have better contact with the vascular wall, which increases the efficiency of the procedure. A significantly smaller amount of sclerosant is needed to achieve results, because it does not dissolve in the blood.
In addition, it does not spread beyond the area of the procedure, which makes it easier to control its strength.
Liquid sclerosants are usually used to remove small varicose veins, while foam preparations allow even large veins to be sclerosed.
Sclerosis of small veins and capillaries is usually performed under visual control, and introduction of foam sclerosant into large blood vessels under ultrasound control.

Miniphlebectomy
This is a minimally invasive surgical method for excision of varicose veins. It does not require any incisions, anesthesia or epidural therapy.
The treatment of this operation is carried out in a day hospital. The doctor performs an ultrasound examination of the blood vessel and marks it with a marker on the skin. After that, he makes a puncture (an incision no larger than 1-2 mm), through which he pulls out a part of the vein with a special hook. This area is compressed and cut off.
Then, the doctor moves on to the next area, makes a puncture, pulls out part of the vein and cuts it. In this way, he removes the entire affected vessel.
Punctures on the skin heal quickly and leave no traces, which achieves an ideal cosmetic effect. The absence of incisions makes the rehabilitation period minimal. Cut veins are not sewn up, and punctures do not require stitches - they are simply sealed with an adhesive patch.
Phlebectomy
It is a classic surgical operation that has been used less and less recently. It consists of radical removal of varicose veins along their entire length. To do this, an incision is made in the groin or below the knee, through which the probe is inserted into the vessel.
With the help of a probe, the vessel is separated from the surrounding tissues and pulled out. The operation is performed under general anesthesia or epidural anesthesia.
Rehabilitation
After treatment of varicose veins, it is necessary to wear compression stockings. The first few days it should be worn 24 hours a day, in the following weeks only during the day, and it can be taken off at night. General restrictions for the rehabilitation period include exclusion of hot baths, steam baths and saunas.
After minimally invasive operations (laser coagulation, radiofrequency ablation, sclerotherapy, miniphlebectomy), it is recommended to get up and walk. In the future, walking is recommended as a mandatory part of the rehabilitation course (at least 1 hour a day), while all other physical activities should be limited.
The duration of the rehabilitation period depends on the extent of treatment and surgical intervention.